Emerging Evidence for the Use of Non-statin Therapies
Statins have been and remain the cornerstone of drug therapy for primary and secondary prevention of atherosclerotic cardiovascular disease (ASCVD) in patients with hypercholesterolemia, including familial hypercholesterolemia. Statins inhibit 3-hydroxy-3-methylglutaryl (HMG)-CoA reductase, a rate-limiting enzyme involved in the synthesis of cholesterol. This leads to upregulation (i.e., increased expression) of low-density lipoprotein (LDL) clearance receptors on hepatocytes, which removes LDL-cholesterol (LDL-C) from the systemic circulation. Four types of patients benefit from statin therapy based on evidence from clinical trials: (1) patients with clinical ASCVD, (2) patients with an LDL-C of 190 mg/dL or higher (many of whom have familial hypercholesterolemia), (3) patients without ASCVD but with type 1 or 2 diabetes mellitus who are 40-75 years old, and (4) patients without ASCVD but with a 10-year estimated risk for ASCVD of 7.5% or higher who are 40-75 years old. However, statin therapy is inadequate or intolerable for some of these patients, and the addition of or substitution with a non-statin may be needed.
This e-newsletter is part of a series of learning opportunities developed by ASHP Advantage related to the role of non-statin therapies in managing patients with hypercholesterolemia, including patients with familial hypercholesterolemia or clinical ASCVD.
Content for this e-newsletter is based in part on participant questions about unresolved issues in the use of non-statins to manage hypercholesterolemia during a live symposium at the 2016 ASHP Midyear Clinical Meeting and Exhibition, as well as an Ask the Experts webinar held on March 1, 2017.
If you missed previous activities, archives of the Midyear symposium and Ask the Experts webinars are now available (ASHP membership is not required, and there is no charge for participation).
New Expert Consensus on Non-Statin Use
The 2013 American College of Cardiology (ACC)/American Heart Association guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults was released before the approval by the Food and Drug Administration (FDA) of the non-statins alirocumab and evolocumab, which are proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors. The ACC Expert Consensus Decision Pathway (ECDP) on the role of non-statin therapies for LDL-C lowering in the management of ASCVD risk released in 2016 provides guidance for clinicians about how to use non-statins to manage patients who are unable to tolerate or have an inadequate LDL-C response to maximally tolerated statins. Non-statins addressed in the ECDP include ezetimibe, bile acid sequestrants (i.e., cholestyramine, colestipol, colesevelam), and the PCSK9 inhibitors alirocumab and evolocumab.
Ezetimibe inhibits intestinal absorption of dietary cholesterol, increasing its excretion. In clinical practice, it is used primarily in combination with statins based largely on data from the Improved Reduction of Outcomes: Vytorin Efficacy International Trial (IMPROVE-IT), although ezetimibe may be used instead of statins in patients unable to tolerate statins. Adding ezetimibe to statin therapy significantly reduced LDL-C and cardiovascular outcomes in patients with acute coronary syndrome in IMPROVE-IT.
Bile acid sequestrants deplete the intrahepatic cholesterol pool by binding bile acids in the gut lumen. This decrease in cholesterol triggers an increase in HMG-CoA reductase expression, which increases LDL-C production. This increase is exceeded, however, by an increase in hepatic LDL clearance receptor activity, resulting in decreased plasma LDL-C levels. As with ezetimibe, bile acid sequestrants may be used for patients unable to tolerate or with an inadequate LDL-C response to maximally tolerated statins. Bile acid sequestrants often are considered after ezetimibe due to a higher risk of gastrointestinal side effects and drug-drug interactions.
According to the ECDP, non-statins should be used only after maximally tolerated statins have been tried. Ezetimibe (or a bile acid sequestrant) should be tried first followed by a PCSK9 inhibitor in patients with clinical ASCVD. In patients with a baseline LDL-C of 190 mg/dL or higher, either ezetimibe or a PCSK9 inhibitor may be added to maximally tolerated statin therapy, with no specified order of preference. Niacin is not recommended. The use of PCSK9 inhibitors is recommended in the ECDP only for patients with ASCVD or a baseline LDL-C of 190 mg/dL or higher, which aligns with the FDA-approved indications for the drugs.
More Information
- Lloyd-Jones DM, Morris PB, Ballantyne CM et al. 2016 ACC expert consensus decision pathway on the role of non-statin therapies for LDL-cholesterol lowering in the management of atherosclerotic cardiovascular disease risk: a report of the American College of Cardiology Task Force on Clinical Expert Consensus Documents. J Am Coll Cardiol. 2016; 68:92-125.
- Stone NJ, Robinson JG, Lichtenstein AH et al. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014; 129(25 Suppl 2):S1-45.
Initiative Faculty

Joseph Saseen, Pharm.D., CLS, BCPS, BCACP, FASHP, FCCP, FNLA, Activity Chair
Professor, Departments of Clinical Pharmacy and Family Medicine
Vice-Chair, Department of Clinical Pharmacy
University of Colorado Anschutz Medical Campus
Aurora, Colorado

Kim K. Birtcher, Pharm.D, M.S., CLS, BCPS-AQ Cardiology, CLS, CDE, AACC, FNLA
Clinical Professor
University of Houston College of Pharmacy
Clinical Pharmacist
Kelsey-Seybold Clinic
Houston, Texas
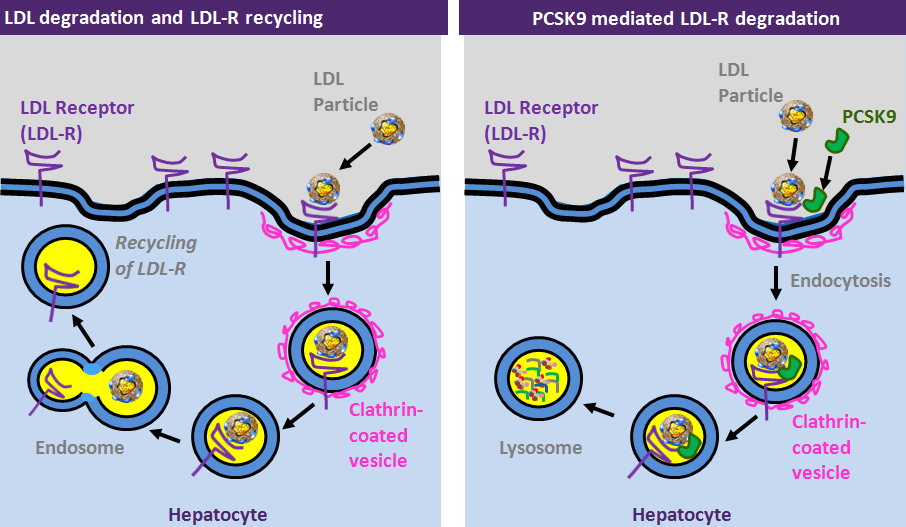
Non-Statin Mechanisms of Action
The LDL clearance receptors on hepatocytes bind LDL particles (i.e., LDL-C) and remove them from the systemic circulation through endocytosis and formation of a clathrin-coated vesicle inside the hepatocyte (Figure). An endosome is formed, the cholesterol is broken down for physiologic use, and the LDL clearance receptor is recycled for use on the hepatocyte surface. When the enzyme PCSK9 is present, it binds to the LDL clearance receptor along with the LDL particle but endocytosis results in formation of a lysosome in which the LDL clearance receptor is broken down along with cholesterol. This interrupts the recycling of LDL clearance receptors, interfering with LDL-C removal from the bloodstream. Monoclonal antibodies were developed to target PCSK9 and extend the process by which LDL clearance receptors are recycled to the hepatocyte surface for continued LDL-C removal from the bloodstream. The two PCSK9 inhibitors approved by FDA to date are alirocumab and evolocumab. Both drugs bind to PCSK9 thereby inhibiting it from binding to the LDL clearance receptor, preventing receptor degradation, and permitting recycling of the receptor to the hepatocyte surface where it can clear LDL-C from the bloodstream and lower LDL-C levels.
Alirocumab and evolocumab are approved by FDA for use as an adjunct to diet and maximally tolerated statin therapy for adults with heterozygous familial hypercholesterolemia or clinical ASCVD who require additional lowering of LDL-C. Evolocumab also is approved as an adjunct to diet and other LDL-lowering therapies (e.g., statins, ezetimibe, LDL apheresis) for patients with homozygous familial hypercholesterolemia. Preliminary findings from large-scale trials and meta-analyses suggest significant reductions in LDL-C, myocardial infarction (MI), and all-cause mortality from the use of PCSK9 inhibitors.
In a phase 3, multicenter, double-blind, randomized, placebo-controlled study of evolocumab known as GLAGOV, coronary atheroma volume was evaluated using intravascular ultrasound in 968 patients with coronary artery disease who were receiving optimized statin therapy. The primary endpoint was change from baseline in percent atheroma volume (PAV) to week 78 compared with placebo, and secondary endpoints were change in normalized total atheroma volume (TAV) and the percentage of patients with plaque regression. A decrease in PAV by 0.95% was associated with evolocumab and an increase by 0.05% was associated with placebo, a difference that is significant (p < 0.001). A significantly larger decrease in TAV was associated with evolocumab (5.8 mm3 vs. 0.9 mm3 with placebo, p < 0.001). Plaque regression was observed in a significantly higher percentage of patients treated with evolocumab than placebo (64.3% vs. 47.3%, p < 0.001). These findings reflect reduction in atherosclerosis in coronary arteries from the addition of evolocumab to maximized statin therapy.
More Information
Game Changing Landmark Study
The ability of PCSK9 inhibitors to reduce the risk of hard cardiovascular endpoints (e.g., MI, stroke) has been a major consideration in the use of these medications because of the high cost of the drugs and the need for long-term therapy. The results of the Further Cardiovascular Outcomes Research with PCSK9 Inhibition in Subjects with Elevated Risk (FOURIER) have been eagerly awaited. This landmark randomized, double-blind, placebo-controlled study of evolocumab involved more than 27,000 patients with ASCVD and LDL-C levels of 70 mg/dL or higher who were receiving optimized statin therapy with or without ezetimibe. The findings were presented at the 2017 ACC 66th Annual Scientific Session and Expo (ACC.17) in Washington, DC, and published in the New England Journal of Medicine in mid-March. The median duration of follow-up was 2.2 years, although 4 years of treatment were planned, because the primary efficacy endpoint (a composite of cardiovascular death, MI, stroke, hospitalization for unstable angina, or coronary revascularization) was reached early. Compared with placebo, the median decrease from baseline in LDL-C after 48 weeks of evolocumab therapy was 59% from 92 mg/dL to 30 mg/dL. A significant 15% reduction in the primary efficacy end point and 20% reduction in a key secondary efficacy end point (a composite of cardiovascular death, MI, or stroke) were observed after 2.2 years of evolocumab treatment. Evolocumab was not associated with a significant reduction in cardiovascular death or death from any cause, but the study was not powered to detect a difference between evolocumab and placebo in these endpoints or the primary endpoint due to the early study termination. The reduction in risk for the primary and key secondary efficacy endpoints increased with increases in the duration of evolocumab therapy. There were no significant differences between evolocumab and placebo in adverse events. The cardiovascular benefit from evolocumab was consistent across a broad range of baseline LDL-C levels and different intensities of statin therapy, regardless of ezetimibe use.
Concerns have been raised about cataracts and neurocognitive adverse effects (e.g., memory loss or impairment, forgetfulness, amnesia, confusion) from the use of statins and PCSK9 inhibitors, possibly related to very low LDL-C levels. Pooled data from 14 controlled clinical trials of alirocumab revealed no significant difference between the alirocumab group and the control group in the incidence of cataracts, but the rate of cataracts was higher in patients with an LDL-C less than 25 mg/dL than in patients with a higher LDL-C. In FOURIER, there was no significant difference between evolocumab-treated patients and placebo-treated patients in the incidence of cataracts. Results of a substudy of cognitive function in 1974 FOURIER participants known as EBBINGHAUS were presented at ACC.17. No significant differences between evolocumab and placebo in cognitive function were found after a mean follow-up time of approximately 19 months, regardless of LDL-C level.
These findings dispel concerns about the safety of very low LDL-C levels and suggest that an LDL-C target lower than what is currently recommended in guidelines is appropriate for patients with ASCVD. The duration of treatment in FOURIER was relatively short (the study was terminated early), so an open-label extension trial to assess the long-term safety of evolocumab is planned for 6000 of the FOURIER participants. The potential benefit from PCSK9 inhibition in a broader patient population at risk for ASCVD with elevated LDL-C levels who do not meet the FOURIER enrollment criteria (e.g., patients at high risk for but without ASCVD) remains to be determined in clinical trials. Nevertheless, the FOURIER and EBBINGHAUS findings are game changing, according to faculty members, Joseph Saseen and Kim Birtcher. According to Dr. Saseen, “long-term data are needed for all new medications, especially PCSK9 inhibitors because of their novel mechanism of action and extended (if not indefinite) period of use in a given patient. The safety and efficacy data available to date for the PCSK9 inhibitors should instill a sense of confidence among clinicians about using these medications. The million dollar question about whether these medications are priced so that they can be used in a cost-effective manner is still unanswered.” Dr. Birtcher noted that “the clinician and patient will need to weigh both the potential ASCVD risk reduction and cost when considering a PCSK9 inhibitor in addition to maximally tolerated statin therapy.”
More Information
- Sabatine MS, Gugliano RP, Keech AC et al. Evolocumab and clinical outcomes in patients with cardiovascular disease. N Engl J Med. 2017; 376:1713-2.
- Dullaart RPF. PCSK9 inhibition to reduce cardiovascular events. N Engl J Med. 2017; 376:1790-1
- Fitzgerald K, White S, Borodovsky A et al. A highly durable RNAi therapeutic inhibitor of PCSK9. N Engl J Med. 2017; 376:41-51.
- Giugliano RP, Mach F, Zavitz K et al. Primary results of EBBINGHAUS, a cognitive study of patients enrolled in the FOURIER trial. American College of Cardiology 2017 Scientific Sessions; March 18, 2017; Washington, DC. Abstract 17-LB-16161-AC.
- Brauser D. No cognitive impairment on evolocumab in EBBINGHAUS study. March 21, 2017. (accessed 2017 Apr 27).
- Clinicaltrials.gov. Evaluating PCSK9 Binding antiBody Influence oN coGnitive HeAlth in High cardiovascUlar Risk Subjects (EBBINGHAUS). (accessed 2017 Apr 11).
In the Pipeline
Other PCSK9 inhibitors are in development. Investigational strategies for targeting PCSK9 include anti-PCSK9 vaccines and inclisiran (formerly known as ALN-PCSsc), which inhibits the synthesis of PCSK9. A phase 2 randomized, double-blind clinical trial known as ORION of inclisiran in patients with ASCVD or risk equivalents, such as diabetes mellitus and familial hypercholesterolemia, and elevated LDL-C levels despite maximally tolerated doses of LDL-lowering therapies, is underway. The recently released results of a preliminary analysis of interim data suggest a significant long-term reduction in LDL-C levels for up to 180 days from 300-mg subcutaneous (s.c.) injections given on day 1 and day 90. An 18-month, phase 3, randomized, placebo-controlled study of inclisiran involving 3000 patients with ASCVD or familial hypercholesterolemia is planned. A 300-mg dose of inclisiran or placebo will be given by s.c. injection on day 1 and day 90, followed by two additional doses every 6 months (i.e., a total of four doses). The primary endpoint will be a composite of coronary heart disease death, non-fatal MI, and fatal and non-fatal ischemic stroke. The results of this and other research involving other therapies targeting PCSK9 are needed to determine the role of these therapies in managing hyperlipidemia.
More Information
- Anon. Trial of investigational PCSK9 synthesis inhibitor for atherosclerotic CVD underway. January 30, 2016. (accessed 2017 Apr 27).
- Anon. LDL lowered, sustained with inclisiran injection in phase 2 study. November 15, 2016. (accessed 2017 Apr 27).
- Anon. The Medicines Company and Alnylam Pharmaceuticals announce agreement with FDA on phase III clinical program for inclisiran. April 26, 2017. (accessed 2017 Apr 27).